
General FAQ
Street nurses is a medico-social organisation convinced that it is possible to end homelessness once and for all in Brussels, Liège and elsewhere. Our organisation contributes to this goal by taking off the streets the most vulnerable homeless people in terms of health, and by mobilising other organisations as well as the general public to find sustainable solutions to the problem of homelessness.
To succeed in rehoming patients for the long-term – homeless people living very precariously – Street nurses uses the following approaches:
- raise awareness of the importance of their health and personal hygiene, and motivate them to take care of these;
- gradually improve self-esteem, including by highlighting people’s qualities and talents;
- work closely with other organisations and institutions, because it is better for the patient to have several points of contact in order to feel that they are being supported. Moreover, efficient and long-term work cannot be done in isolation;
- create housing.
Street nurses seeks to kindle enthusiasm, to get the general public involved, and to work in an innovative way to put an end to homelessness.
Street nurses provides training for professionals: born out of a recognised need in the sector, this sharing of experience and expertise is a way to extend our impact on society.
Street nurses also shares its experience and expertise with professionals by welcoming Belgian and European organisations, and by taking part at exchange programmes in Europe and elsewhere.
Trust towards others
First, we try to gain their trust be creating a relationship. Once the homeless person starts to trust us, we help him or her to understand the importance of a good personal hygiene. We devote the time needed, we respect his rhythm, but we do not ever give up on that person – and we keep going until this person allows us to enter his world. This can take months.
Hygiene and health
To agree to have a shower, to see a doctor, or just to accept to wash his or hands…every little step is important, because little by little, the patient learns to respect himself again, and to have faith in himself, which is essential for this person to dare to imagine him or herself living in an accommodation again. It’s our job to help them to make that happen!
Self-esteem, self-confidence
From the beginning, we make sure to raise their awareness of their talents/abilities, of their qualities and the activities that they enjoy (music, walking in nature, cooking, etc.), always with the intention to stimulate a will to live, and self-esteem.
Administration
Not having an identity card or address, the loss of social rights…sorting out the person’s administrative existence takes a lot of time and energy that they no longer have: we provide them with administrative and legal support.
Accommodation
Once re-housed (which can happen very quickly, but can also take several years – the average duration is 1.5 years), we continue to follow our patients closely until the moment when they become independent, and even after this point. In addition, a volunteer visitor visits regularly – for a simple visit, for a coffee, to play chess or to go for a walk.
Several criteria are taken into account, such as: immobility (if the person stays at the same spot on the streets most of his time), age, if the person has let him or herself go, mental and physical health, the existence or not of a social network, the number of years spent homeless (we used to focus on people who had spent 8 years or more on the streets, now we work with those who have spent 3 years or more being homeless, because the more serious cases have been taken off the streets), gender etc.
We do not ignore the homeless people that we are unable to take care of: on the contrary, we register information about them, we look for other organisations that can help them out, and go back to them once we have a free spot. We always work with a network made of social and medical institutions and actors in Brussels.
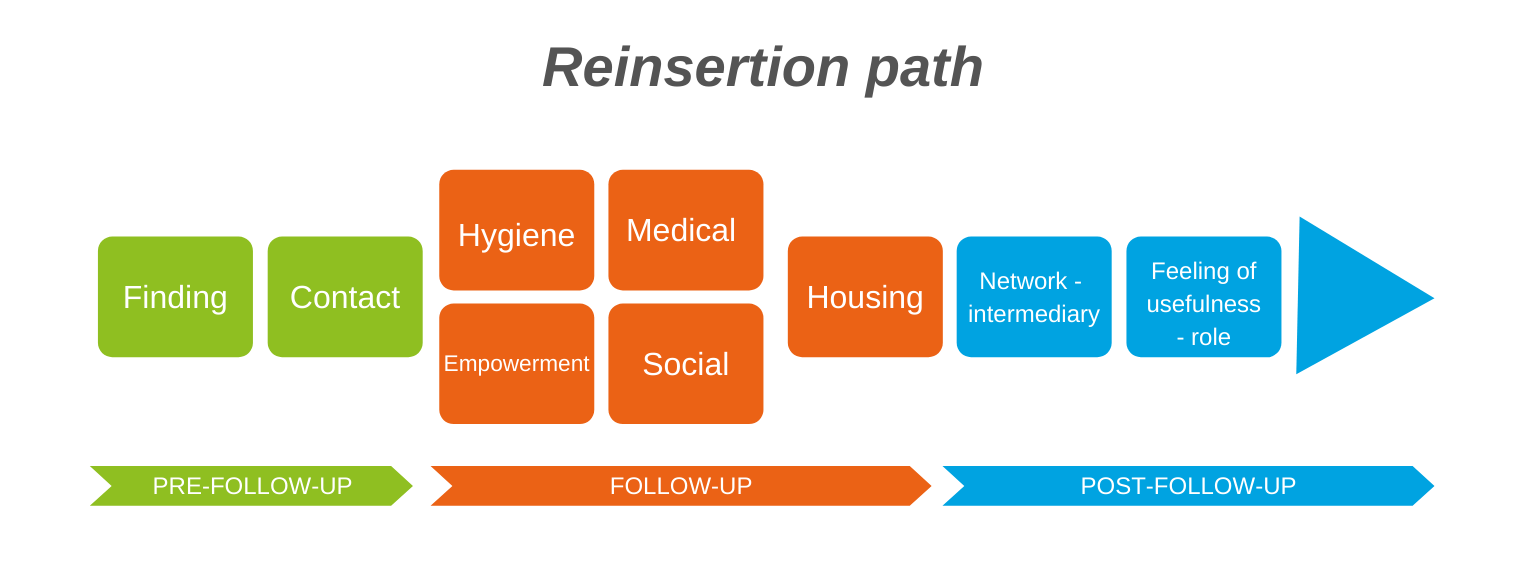
These terms indicate in which phase we are currently while taking care of the patient.
Pre-follow-up
This is the phase in which we register all of the people that our network and individuals have reported to us. A homeless person is cared for by our teams out of the field if they are considered particularly vulnerable, and on the basis of various objective criteria.
Follow-up
Care means carefully looking after the person – this is the core of our work. It starts in the streets and continues until the patient is placed in accommodation where he or she will continue to benefit from support from professionals and Street nurses’ volunteers regularly, but less frequently. This avoids a relapse and a return to the streets.
Find out more about how we take care of
our patients living on the streets
Follow-up in accommodation
We do more than simply take care of moving these people from the streets to stable accommodation. Once the patients have been rehomed, we continue to follow them closely for a while.
Find out more about follow-up in accommodation
Post-follow-up in accommodation
In the first 10 years of our organisation’s work, we took people off the streets who had been surviving there for eight years or more (between 8 and 25 years). These were extremely vulnerable people, with very complex problems. Those working in the medical and social sector had given up hope that these people would ever live in accommodations.
The steps for the patients take time.
Trust the team
Get back into good health
- Take care of themselves, register with a medical provider, take medication as necessary, follow treatment, etc.
Regain confidence in themselves, re-establish self-esteem
Sort out their administrative situation.
- Sorting out the patient’s administrative situation (ID card, social rights) can, in some cases, take a lot of time and requires, in certain cases, contact with lawyers.
Arrival in accommodation.
- This last step is not in the patient’s hands. Once the patient wants to get off the streets and has his documents in order, accommodation must be available. The number of people that we can take off the streets has a direct link to the number of places available in accommodation. Due to a lack of housing in Brussels – which is by the way considerable – there were 16 places in 2019. Street nurses is launching innovating pilot projects to find new types of accommodations for the most vulnerable people.
Living in accommodations.
- We do more than simply moving these people from the streets to stable accommodations. Once the patients have been rehomed, we continue to follow them closely for a long time. In addition, we run campaigns and work to raise awareness about the problem of homelessness.
We aspire to live in a society in which there are no longer homeless people. Homelessness should be an extraordinary situation, the result of an emergency, and not structural. We are really convinced that homelessness is avoidable, neither for the person concerned, nor for the society. Nobody sleeps on the streets because they want it. The average life expectancy for one living on the streets is 47 years, compared to an expectation of 80 for the Belgian population at large. We are convinced that for every marginalised, homeless person, there is a way to obtain (and they have a right to) support and above all, find an appropriate accommodation that allows them to leave the streets permanently. We believe that every individual has the qualities and talents needed to find a place in society.
Our ambition is to banish structural homelessness from Brussels by the end of 2025 by bringing together the world of politics, citizens, businesses and other investors. We want a world in which everyone lives in dignified and secure conditions. And we want to prove that this is possible in Brussels, and to make Brussels an example for Belgium, as well as for other countries.
Working within a network is crucial for efficiency. Moreover, for the patient, a network is essential because it is linked to a network of organizations and people that will support the person; he will feel less alone and will be able to ask for help.
Our network comprises around 100 organizations and institutions. Every organisation working in this area has its own specific approach and its own role. Patients are often cared for by a series of organisations at the same time. For that reason, we constantly need to be in touch with the different organisations and support groups.
Every organisation has a different goal, and deals with the problems differently. Here are a few examples:
- L’Ilot takes care of moving homeless people into sheltered accommodation
- SAMU social works night and day and has emergency shelters
- If an accommodation becomes available, the different organisations contact one another to determine which patient has the greatest need.
- Some organisations focus more on families or young people.
We are in touch with movements advocating the end of homelessness in Europe, and elsewhere such as in the United States or in Japan, in order to share our expertise and to learn from solutions put in place outside of Brussels. These discussions are important for innovation, to question our work, and to motivate us in our daily fight against hardship.
For the homelessness problem in Brussels, nobody has an obvious overview, or one which provides the relevant facts and figures. Different factors and causes play a role. The reasons why someone is on the streets can be numerous: an illness, the breakdown of a relationship, redundancy, bankruptcy etc. But one thing that all cases have in common is the absence of a support network. They find themselves alone.
The economic situation for everyone, the lack of a social security net, the lack of medical care (for physical and mental health) and migration are some of the factors playing a role in the rise of homelessness.
Among those who sleep outside, we see old and young people, men and women. Often, priority for accommodation depends on how vulnerable a person is. The survey of the 2017 campaign 400 Toits (‘400 rooves’) showed that 12% of the people on the streets were women. Living on the streets is even more dangerous for women. Often, they are prioritised for emergency accommodation, because of their bigger vulnerability. But as many women as men, say that their situation has been caused by a traumatic event (36%).
In 2017, more than a quarter of those identified for a survey were aged under 35, 7% were older than 60. The age group that is most represented is the 46-59 year olds, who accounted for 34% of the participants.
Ultimately, it’s your choice: money, something to eat or drink, or some other item. It is important that you feel comfortable with your choice.
If you want to offer someone something to eat, it is perhaps best to first ask him or her what he or she would like to eat or drink. This will ensure you to avoid difficult situations. Here are two examples: an apple could be rejected because the person in question no longer has any (healthy) teeth to eat it; and a ham sandwich may be rejected by a Muslim. We all have the right to say that we don’t want to give certain things, like alcohol.
Giving money to someone also gives him or her the freedom and the responsibility to make his or her own choices about how to spend the money.
We do look after people with mental health problems, but we try to limit the number of patients in that category because taking care of them is a long and difficult process. For the wellbeing and motivation of the team out on the field, we need to pay attention to this.
Undocumented people are often those with mental health problems, so we limit the number of undocumented people we work with. The process to get documents in order is long and tiring, and we want our team to remain motivated and dynamic. We do have a staff with expertise in this area, but these people are not especially our target group. Our target group are the most vulnerable people. It is however true that among the most vulnerable people, we are finding more and more undocumented people.
We organise training for those working in the medico-social sector who were put off, or afraid to talk about hygiene with homeless people.
At the moment (2023), the organisation has more than 50 paid employees, including, of course, a doctor and nurses. There are also social workers, a psychologist, educators, experts in housing and logistics, people responsible for lobbying, communication and fundraising. And, of course, we have a number of staff members who ensure that the financial management and administration run smoothly and professionally.
We are always open for volunteers.
FAQ street work
We decide, using our own tools, whether a person ‘belongs’ to our target audience. If you want to alert us to a vulnerable person, you can contact us. Depending on how urgent the situation is, we may direct you to other organisations, and/or one of our teams may go and assess the situation. However, due to our workload, we cannot guarantee that we will be able to come and take a look immediately.
As of right now, we are taking care of around 100 patients.
The average amount of time needed to take someone off the streets, from the first contact to genuine rehousing, at least around 1.5 years. However, we work with some patients for many years, while we are able to rehouse others within just a few months.
That varies from patient to patient and depends on their needs. We see lots of patients every week.
First, we generally need to sort out their identity documents.
Then we look into the options for obtaining income from the CPAS (public welfare office), health insurance, pension funds, the unemployment office or other sources. This means a series of appointments and processes.
Finally, once the person has been housed, we need to take care of the rental guarantee: either the person in question or the CPAS should provide the sum required.
During the first wave, lots of homeless people didn’t understand why, all of a sudden, the streets were empty. They had to adapt. Many suffered, as they no longer had anyone to ask for a few coins, and the snack bars where they usually go to, to ask for free food or drinks were closed. Many were therefore thirsty and hungry.
While waiting for other services to adapt how they worked and (re)launch their activities, we had to compensate for what was missing by distributing food and even water, as well as personal protection equipment, and even to raise awareness of how to avoid contracting the virus. We also took care for those lodged in hotels, carrying out medical visits twice a week.
FAQ Work in housing
We decide in a meeting which patients will go to which accommodation. Our decision is based on their degree of vulnerability, but also on the characteristics of the accommodation available: the neighbourhood where it is located, the logistics related to the accommodation (floor, lift,...).
As soon as we can shelter people, we do. Either in emergency accommodation or in medium-term accommodation (hostels). The search for a more sustainable solution then takes place during the stay in emergency accommodation. It so happens that these forms of accommodation are not very accessible for our patients, either because the conditions of access are too restrictive (special hours, abstinence, little time for reflection, etc.) or because the living conditions are too harsh (violence, theft, parasites, etc.) and our patients still refuse to go there.
Yes, we still follow the re-housed patient. When the patient slept on the street, he lived surrounded by a lot of people. Although this situation was very psychologically difficult, suddenly being alone in his or her own home can be destabilising at first.
Once the patient is stabilised and independent, we continue to visit him.
The follow-up ends 10 years after the patient has been stabilised in his or her home. During this period, the follow-up can be reduced to maintaining contact, to make sure that everything is going well, and to keep information about the patient's state of health. The idea is to keep track of the impact of the years of life on the streets on the long-term (10 years) survival and health of people. The other usefulness of this long term monitoring is to prevent people from returning to the streets, by being able to intervene, if the situation deteriorates, before a loss of housing. It is also a guarantee for our network partners, to whom we entrust the follow-up of our patients: they know that they can call us in case of problems, even years later.
In Brussels, there is a serious lack of housing. Our organisation has a dedicated team called "housing creator and housing collector" that goes out to find housing for our patients. We find individual housing (which we usually manage through Social Real Estate Agencies) or collective housing (nursing homes, retirement homes).
We are also looking for completely innovative solutions: in 2018 we installed a modular housing unit that can be moved to a piece of fallow land (therefore less expensive because the land does not have to be bought) and we hope to interest the public authorities and investors in order to buy others and to have other fallow lands that can be used temporarily, from 2 to several years.
At the moment, our biggest partners for re-housing are clearly the AIS (almost all re-housing, and certainly all re-housing directly from the street), even if their rents are higher than in social housing.
We have more easily places in AIS, there is still more support and tolerance for our patients, and when the person loses their housing, this housing is not lost to the organization, which can immediately rehouse someone else in this housing. Social housing is cheaper but has long waiting times (at least a few years), it is much more procedural and less tolerant, and the housing is granted on an individual basis: if the person is evicted, the housing is lost to the project.
We have given up working directly with private landlords, because in all cases this does not go well. The direct confrontation between the landlord and the concrete problems encountered in the housing (degradation, neighbourhood disturbances) make long-term success impossible in most cases.
Some patients have found a real job. Others do voluntary work in order to stay active once they are in housing.
But our patients are a very specific target group who often are or have become very vulnerable after a long stay on the streets. Or who are confronted with severe problems, both physical and mental, so that a reintroduction into the regular work circuit is not always easy. If possible, we work together with more specialised organisations in order to be able to offer career guidance or therapy aimed at re-education.
Clichés about homeless people
Surviving on the streets for years, makes you believe that this situation will never change.
Many factors affect willpower and clarity of mind: fatigue (4 hours of sleep per night sectioned in 10-minute periods), poor physical health, depression, poor diet, not to mention alcohol or drugs that make it possible to forget the daily difficulties.
To avoid again another disappointment or failure, people prefer to withdraw from themselves and others, and will refuse any form of assistance. For that reason, it is important to gradually gain their confidence and to restore their conviction that getting off the street is possible!
Thanks to an adapted support, allowing time, respecting the rhythm, and without ever giving up on the person or abandoning our final goal, even patients who were living for 15 to 20 years on the street ended up wishing for housing.
No one chooses this option. One day you find yourself on the street because of a combination of circumstances and because there is no one left in your network (family, friends) who can help you. Living on the street is extremely difficult, and it quickly damages your physical and mental health!
This figure speaks for itself: an average life expectancy is around 47 years for homeless people, compared to a life expectancy of more than 80 years for the average Belgian population.
The major problems encountered in the streets, according to the homeless people themselves, are the lack of privacy and the lack of security (constant fear of being robbed or assaulted, asking them to be on the alert 24/7). The issues of hunger and lack of water come next.
To live again in any kind of housing, after all these years on the street, means a radical change. A rehoused patient may begin by sleeping on the floor instead of going to bed. A period of transition and adaptation is normal. But in the end, they all end up appreciating and cherishing the new comfort and especially the security of a home.
At the beginning, in general, when they think about housing, they absolutely want individual housing (finally alone!), but a certain number of rehoused people end up asking to move to a collective housing (roommate, retirement home, etc.) because loneliness is too difficult to manage. Nevertheless, this move to a single apartment was an essential step, because they would not have accepted a collective apartment from the start.
Although alcohol, drugs, and other addictions are common among homeless people, this is not a generalization.
If the person consumes, it is often difficult to determine the causes, which are often multiple (fighting the cold, forgetting about their problems, group influence, addiction, boredom, etc.). Getting back in control of one's situation, the concretization of certain projects/objectives such as entering housing can positively influence consumption, or even reduce or stop it.
The street is not a good place to stop these addictions. This is why the Housing First program, which is being developed in many countries and in which Street Nurses participate, does not impose withdrawal before entering housing.
For homeless people, begging is a survival strategy. Begging gives them a bit of money to buy something which, at a particular moment, is important to them.
That can be taking a shower, or a meal in a social restaurant. It can differ from day to day. And they could also buy alcohol and tobacco, or any other product that matters to them then and there – to tolerate their life or manage their stress.
Some beg out of a need for social contact because life on the street is often full of solitude. For others it’s a real job, with working hours to be respected. But for homeless people, begging is an ordeal which fills them with shame but which they cannot do without.
If you find it difficult to give money, you can always ask them what would give them pleasure and then buy that for them yourself. No problem saying then that you’d rather give something else than, for instance, alcohol or cigarettes.
Homeless people form a very mixed group. Their personalities and characters are very different, like in the overall population. Some are shy, introvert, polite, friendly, funny, discrete, whereas others behave extravagantly, incoherently, and come across as strange, even threatening. This is mainly due to the situation in which they live, their physical or mental state of health, and their life on the street.
The latter is very stressful and dangerous. 50% of homeless people say that they have already been attacked and not only by other homeless people. Patients tell us that evenings with matches or festivities are the riskier ones.
Their sleep is also curtailed, on average 4 hours a night, at 10 minutes intervals. They must constantly be on guard against being robbed. In addition, alcohol and mental health problems feed distrust (or even paranoia) of passers-by and even field workers.
For all these reasons, homeless people can appear to be aggressive, even if in most cases they are completely harmless.
At some of our meetings, we are confronted with rejection or fits of rage because we didn’t come at the right moment. We accept that these people express their feelings and then propose to return later.
In our work we can spend on people whatever time is necessary and act outside the box. Thus, we can adapt ourselves to them, respect their rhythm and listen carefully to what they need.
Life on the street is fatal in any season.
If emergency shelters are organized during winter, this season is not necessarily the most dangerous. In spring, however, most emergency shelters are closed, putting hundreds of people back on the street with all its consequences (confusion, isolation, etc.).
In addition, most homeless people suffer from physical and mental problems throughout the year, making them vulnerable in any season.
During heat waves in summer these people run the risks of dehydration and heart problems, which are dangerous if not taken care of on time.
Like during other seasons, we stand ready to help with an eye on specific dangers.
During the winter, cold is the biggest danger with hypothermia as the most frequent risk. Frostbite, possibly with subsequent amputation is another, less recurrent, risk.
To avoid such accidents, we developed two preventive tools: the poster “Cold” and the information sheet “Hypothermia” (to be downloaded on our website).
Following are the three recommendations we’d like to give to the public:
- Don’t give homeless people tea of coffee; these drinks, like alcohol, stimulate heat loss and act as diuretics. Better give another warm drink, such as soup or chocolate.
- Symptoms of light hypothermia are easily recognizable (trembling, confusion, uncoordinated walking), but those of severe hypothermia are often ignored: acting incoherently, refusing help, abnormal behaviour, no trembling, loss of consciousness…
- If you think you’re dealing with a case of severe hypothermia, you best call an ambulance (100). Warming up must be done progressively, little by little, in a medical center. Warming up too fast can be dangerous.
At Street Nurses, we do everything to get our homeless patients connected to a medical center or a general practitioner and thus make sure that their health is looked after in the best place and the long term. Even if we happen to give care to people in the street, we do so in the first place to create a bond of trust. What matters most is to make them active citizens again who over time move into a home of their own – which is the only way to improve physical and mental health.